

In my consulting work, I have provided independent medical/legal assessments of seniors regarding capacity to sign powers of attorney, capacity to manage property and personal care, capacity to marry, capacity to provide instructions, capacity to provide evidence and both retrospective and contemporaneous assessments of testamentary capacity and capacity to provide inter vivos gifts. I have been accredited as an expert witness in contemporaneous and retrospective assessments by the Ontario Superior Court of Justice in John Gironda et al. v. Vito Gironda et al. (2013 ONSC) and Foley v. McIntyre (2014 ONSC). I am not an assessor of the Ministry of the Attorney General. In my clinical work I am a Geriatric Psychiatrist.
Many readers may not be familiar with Geriatric Psychiatry since we are a relatively new subspecialty, only having received formal recognition by the Royal College of Physicians and Surgeons of Canada in 2013. Readers may wonder what kind of expertise is required in order to provide contemporaneous and retrospective capacity evaluations. To this I provide the following summary of Geriatric Psychiatry which, in my opinion, is a field of Medicine comprised of 10 essential clinical issues. These are:
- dementia,
- depression,
- delirium,
- disabling medical illness,
- drugs,
- disconnections (social),
- delusions,
- decision-making capacity,
- discharge planning, and
- death
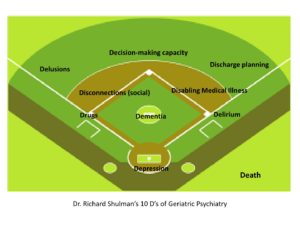
The clinical concepts can be presented schematically like a team of players on a baseball field as shown in the accompanying diagram – the positions on the baseball field correspond to the positions in the list above (for those familiar with baseball scoring and with death in the dugout).
These considerations are pertinent to any assessment, either contemporaneously or retrospectively, of a senior. For example, dementia predisposes one to depression and delirium, is associated with disabling medical illnesses like stroke or Parkinson’s disease, makes a senior more vulnerable to the effects of drugs, predisposes one to either social reliance on others or social disconnections from others, is a common cause for delusions, impacts decision-making capacity, complicates discharge planning from hospital, and ultimately results in death, requiring end-of-life planning.
I could easily address similar connections with any of the other eight as the primary issue. For seniors, death is ultimately the last issue (the one waiting in the dugout (pun intended) in the baseball schematic).
The role of a Geriatric Psychiatrist is to expertly assess and manage these 10 interacting clinical issues as a means to pursue improving or maintaining quality of life as much as possible without contributing to unnecessary suffering for the patient and caregiver.
0 Comments